The principle of distraction osteogenesis is a well-known principle since many decades.
It is important, in my opinion, to distinguish between the principles and the methods of limb lengthening. Limb lengthening uitilizes the principle of distraction osteogenesis (DO). The (DO) principle is applied with different methods. Although the principle of distraction osteogenesis remained unchanged, the methods and devices of fixing the bone and controlling the distraction have evolved through the years. Ilizarov initially used an external circular frame to fix the bone and to control its distraction and external ring fixators have been the only option of fixation until the late 1990’s when intramedullary nails start to be introduced. The methods of applying the principle of (DO) are better discribed in the article Methods of Bone Fixation in Limb Lengthening
DO was first discovered in the 1950’s by Professor Gavril Ilizarov in the former Soviet Union. Because of the political isolation in the years of the Cold war, it wasn’t until the 1980’s that the principle was introduced to the West.
The principle dictates that when a long bone is carefully broken (osteotomized) by the surgeon and the two parts of the bone are then slowly pushed away from each other (distracted), with a rate of around 1mm per day, normal bone is gradually formed in the developing gap. The bone eventually heals in an elongated position.
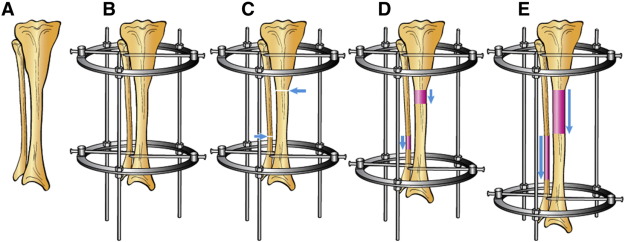
A: Before, B: Fixation of bone, C: Osteotomy, D and E: Distraction
The soft tissues (i.e. skin, muscles, nerves, vessels) also respond to the continuous tension and and they gradually elongate and adapt. Because the lengthening occurs in all tissues and not just the bone, the term “histogenesis” is used by some surgeons instead of “osteogenesis” (“histo-” means “tissue” in Greek).
Distraction osteogenesis is basically intervening and harnessing a natural healing response of the human body ( i.e. the ability of a broken bone to heal) and directing it towards a desired outcome with the help of human-made means.
Many parameters affect the outcome of the distraction osteogenesis and have been being studied continuously through the years. Some of those parameters are:
- The rate of daily lengthening.
- The surgical technique of the osteotomy.
- The location of the osteotomy.
- The condition of the soft tissue around the bone.
- The effect of growth factors, hormones and medications.
- The type and mechanical properties of the fixation.
- The patient’s compliance.
These parameters are discussed below, in the relevant phases of DO: