If you are suffering from or more of the following conditions, limb lengthening surgery may be indicated for you:
Indications for Limb Lengthening
Author: Dimitrios Giotikas MD, PhD
Post-traumatic limb length discrepancy is not uncommon after high-energy injuries are fixed in a shortened position secondary to bone loss. Some studies suggest that leg length discrepancy (LLD) is associated with low back pain and other functional problems. Small post traumatic LLD’s up to 2 cm can be often treated with simple means such as high heel shoes or insoles. Surgical correction may be indicated if the length discrepancy causes significant functional problems such as an abnormal walking pattern and/or persistent, refractory pain in the back, hip or knee.
References
- Kosuge DD, Pugh H, Timms A, Barry M.J. Limb lengthening for post-traumatic shortening over a pre-implanted femoral locking plate. J Orthop Trauma. 2013 Mar;27(3):e57-64. doi: 10.1097/BOT.0b013e3182604558.
- Maffulli N, Lombari C, Matarazzo L, Nele U, Pagnotta G, Fixsen JA. A review of 240 patients undergoing distraction osteogenesis for congenital post-traumatic or postinfective lower limb length discrepancy.J Am Coll Surg. 1996 May;182(5):394-402.
- Rannisto S, Okuloff A, Uitti J, Paananen M, Rannisto PH, Malmivaara A, and Karppinen J. Leg-length discrepancy is associated with low back pain among those who must stand while workingBMC Musculoskelet Disord. 2015; 16: 110.
Achondroplasia is a genetic disorder that results in what is called “disproportionate dwarfism”. In those with the condition, the arms and legs are short, while the torso is typically of normal length. In some cases spinal stenosis may occur. All people with achondroplasia have short stature. The disorder occurs in approximately 1 in 25,000 live births. It’s equally common in males and females.
The average height of an adult male with achondroplasia is 131 centimeters (4 feet, 4 inches), and the average height for adult females is 124 centimeters (4 feet, 1 inch).
Limb lengthening in cases of achondroplasia aims to: increase stature, correct limb deformities, improve interaction with the surroundings (reach, use of furniture, driving etc) and restore body proportions.
The interventions ideally start in childhood from the age of 8 years and, with repeated procedures, atotal height increase of 35 to 40 cm can be achieved.
References
- Cattaneo R, Villa A, Catagni M, et al. Limb lengthening in achondroplasia by Ilizarov’s method. Int Orthop. 1988;12:173–179.
- https://ghr.nlm.nih.gov/condition/achondroplasia#
- Correll J, Held P. Limb lengthening in dwarfism. Orthopade. 2000; 29:787–794.
- Aldegheri R, Dall’Oca C. Limb lengthening in short stature patients. J Pediatr Orthop B. 2001;10:238–247.
It has been agreed by consensus that “Constitutional short stature” is a condition in which the height of an individual is more than 2 standard deviations (SD) below the corresponding mean height for a given age, sex, and population group without evidence of systemic, endocrine, nutritional, or genetic diseases.
In order to better understand what that means, let’s elaborate further on
standard deviation and the mean height.
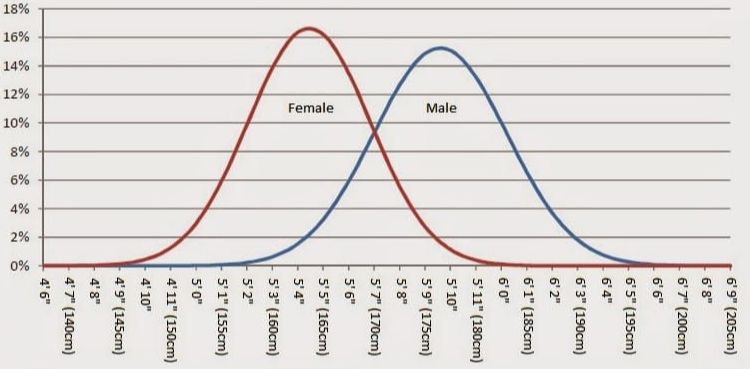
When assessing the distribution of height in a population, we observe that it follows the normal Bell curve (Fig 1).
Fig.1This means the majority of the individuals of the population are closer to the mean average height (peak of the curve) and progressively fewer numbers of individuals have shorter or taller (deviation) height than that average height. In fig. 1, we see that the average (mean) height is approximately 5’4” in females and 5’10” in males. (The mean value varies between human races; this chart refers to Caucasians.)
In statistics, one standard deviation (1 SD) away from the mean value (in our
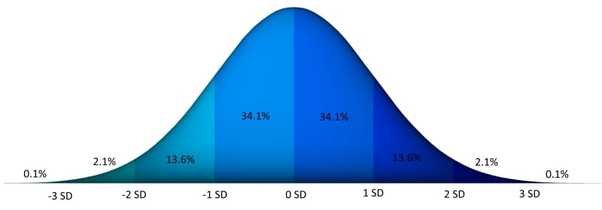
case the mean height) in either direction on the horizontal axis (the two shaded areas closest to the peak of the curve on the graph of fig 2.) accounts for approximately 68 percent of the people (fig 2). Two standard deviations away from the mean (the four areas closest to the peak) account for roughly 96 percent of the people.[4]
Fig.2Normal height is considered any height within 2 standard deviations (SD) from the mean. Short stature is any height below – 2SD. In Caucasian populations, the lower limit of so-called “normal stature” is 5’5” (166cm) for males and 5’0” (153cm) for females.
References
1. Cohen P, Rogol AD, Deal CL, et al. Consensus statement on the diagnosis and treatment of children with idiopathic short stature: a summary of the Growth Hormone Research Society, the Lawson Wilkins Pediatric Endocrine Society, and the European Society for Paediatric Endocrinology Workshop. J Clin Endocrinol Metab. 2008 Nov. 93(11):4210-7.
2. Ranke MB. Towards a consensus on the definition of idiopathic short stature. Horm Res 1996 45(Suppl 2):64–66
3. .Sultan M, Afzal M, Qureshi SM, et al. Etiology of short stature in children. J Coll Physicians Surg Pak. 2008 Aug. 18(8):493-7.
4. https://en.wikipedia.org/wiki/Standard_deviation#cite_note-StatNotes-1
5. https://www.disabled-world.com/artman/publish/height-chart.shtml
If you are genuinely unhappy because you think that you are not tall enough and would like to be a little taller, you might suffer from a condition called height dysphoria or height neurosis.
Height dysphoria or height neurosis is a term that refers to a body image disorder where the patient is unhappy and distressed because they either are short or perceive themselves as short. It is worth noting that this may be irrespective of the actual height and irrespective of how other people see them. Although there isn’t available data about its prevalence, it is considered to be a relatively common condition.
Some cases of height dysphoria are related to cultural and societal norms and expectations while some others are career related. Careers pathways like show-business, modelling, police and military work require confidence, and people ask for the confidence boost of a height lengthening procedure.
Candidates for cosmetic procedures, including cosmetic limb lengthening, do not have a functional problem and they resort to surgical solutions to manage the psychosocial burden of their body variations. This means that in some cases, patients need to be psychologically evaluated to exclude a more severe obsessive mental condition which is called body dysmorphic disorder or a psychosis before a cosmetic procedure is undertaken. This is particularly important for height lengthening procedures, where the complexity and duration of the treatment poses significant mental and physical challenges to patients.
References
1. Horney, Karen (1950). Neurosis and Human Growth: The Struggle Toward Self-Realization. W.W. Norton & Company
2. Ranke MB. Towards a consensus on the definition of idiopathic short stature. Horm Res 1996 45(Suppl 2):64–66
“Hypoplasia” means “not well or fully formed or developed”. There are certain congenital conditions which cause limb deformity and length discrepancy which may be amenable to limb lengthening surgery.
Fibular hemimelia is the most common deficiency of long bones (1/40000 live births) and includes a wide spectrum of congenital anomalies, ranging from mild fibular shortening to complete absence of fibula, and associated defects of the femur, tibia, ankle and foot. It is often associated with shortening of the femur in severe cases. It usually presents clinically as limb length discrepancy, anteromedial bowing of tibia, valgus deformity of the knee, equinovalgus deformities of the foot and ankle, and absent lateral rays
Proximal focal femoral deficiency (PFFD) is part of a spectrum of congenital deformities affecting the femur.
It may range from simple shortening of a normal-appearing femur to the complete absence of the proximal two-thirds of the bone. Deficiencies of the hip and knee joint often coexist and are determinants for treatment.
Treatment is complex and should be undertaken in specialized centers with experience in congenital deformities. Nearly all patients require some combination of surgical and orthotic treatment.Complex reconstruction and limb-lengthening up to 25-30 cm is possible for patients with reconstructable hip and knee joints.
References
- Changulani, F. Ali, E. Mulgrew, J. B. Day, and M. Zenios. Outcome of limb lengthening in fibular hemimelia and a functional foot. J Child Orthop. 2010 Dec; 4(6): 519–524.
- Daniel E. Prince, John E. Herzenberg, Shawn C. Standard, and Dror Paley. Lengthening With External Fixation Is Effective in Congenital Femoral Deficiency Clin Orthop Relat Res. 2015 Oct; 473(10): 3261–3271.
- https://posna.org/Physician-Education/Study-Guide/Congenital-Femoral-Deficiency-(Proximal-Femoral-Fo
Go back to Limb Lengthening- introduction